
🔻臨床WEBサービス「forPT ONLINE」無料体験実施中!🔻
第7頚椎棘突起
椎体で最も突出する棘突起は一般的に第7頚椎(C7)とされ、隆椎(Vertebra prominens:VP)とも呼ばれています(図1)。
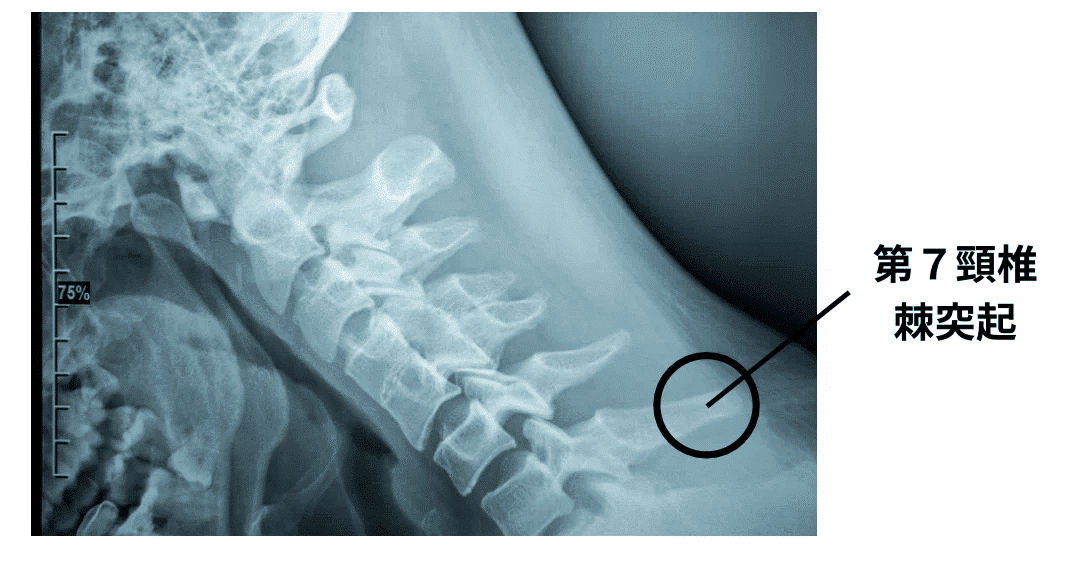
図1 頚椎のレントゲン画像
死体解剖の触診研究では、椎体で最も突出する棘突起は、C7が約49%、C6が約36%、C5が約10%、T1が約5%と大きな個体差がある¹⁾ことが報告されています(図2、図3)。
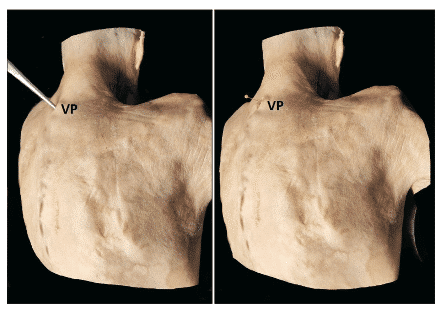
図2 隆椎(VP)
1)より画像引用
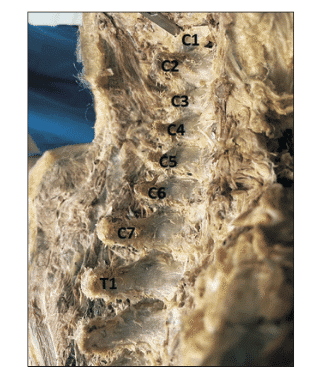
図3 VPがT1の例
1)より画像引用
🎥頚椎棘突起の触診
肩甲骨
肩甲骨上角
肩甲骨の上角は、およそ第2胸椎(T2)高位と一致するとされます(図4)。
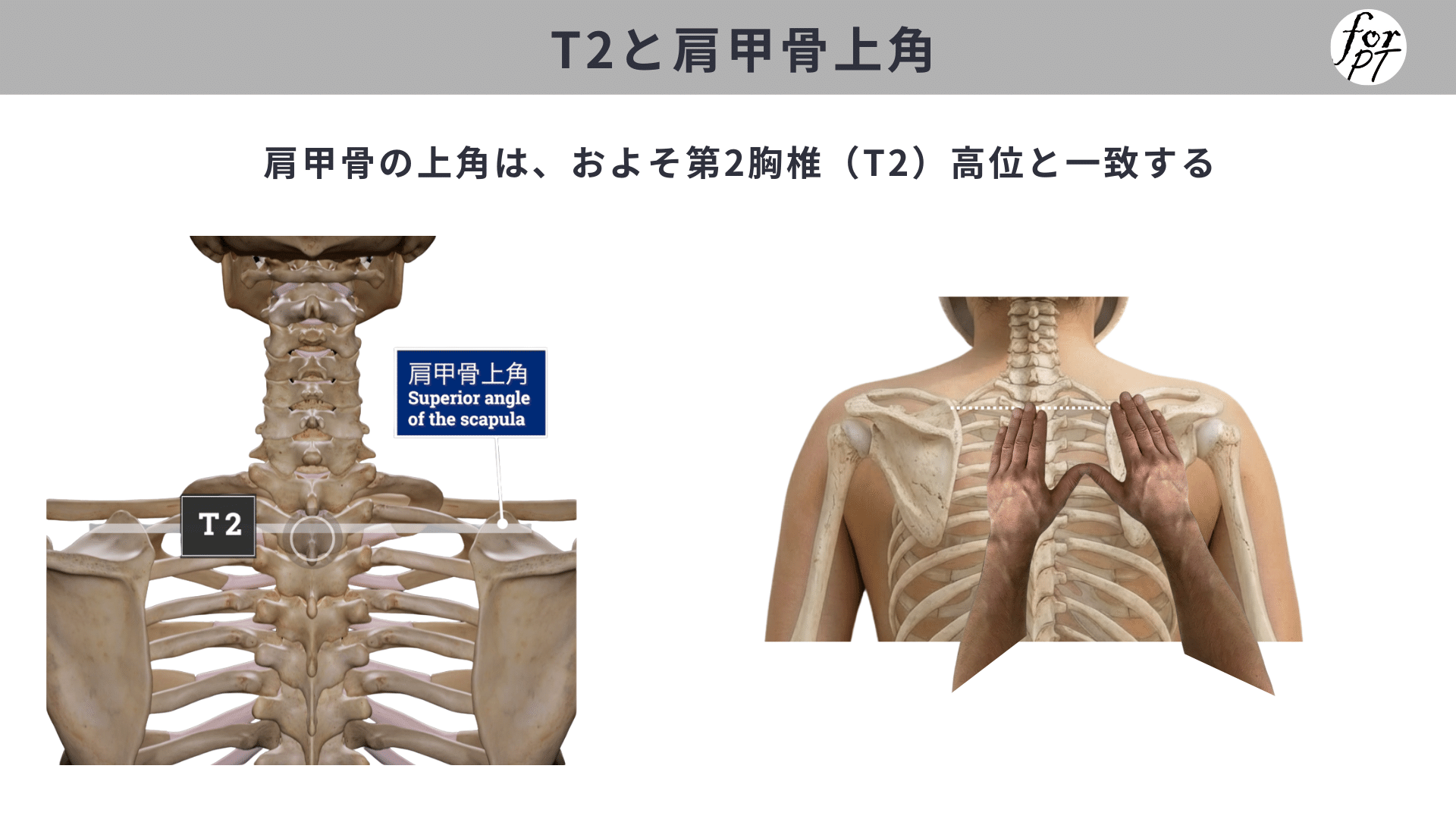
図4 肩甲骨上角とT2
肩甲骨の上角位置が、T2より下方(T3以下)に位置する場合を肩甲骨下制位と定義する研究調査²⁾があります(図5)。
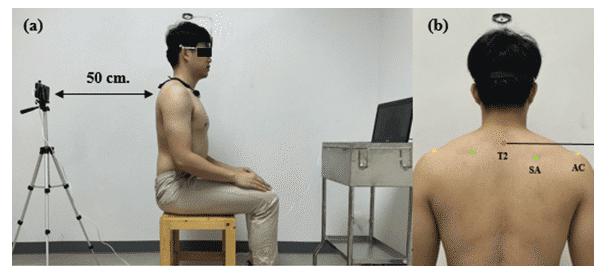
図5 肩甲骨下制位
(T2:第2胸椎、SA:肩甲棘、AC:肩峰)
2)より画像引用
同調査では、慢性頚部痛+肩甲骨下制位の対象者に対して、肩甲骨の能動的な修正運動を行った結果、即時的に頸部回旋ROMを改善し、最大回旋時の頸部痛を軽減した²⁾と報告されています。
肩甲棘の内側端
肩甲骨の内側端は、およそ第3胸椎(T3)高位と一致する³⁾とされます(図5、図6)。
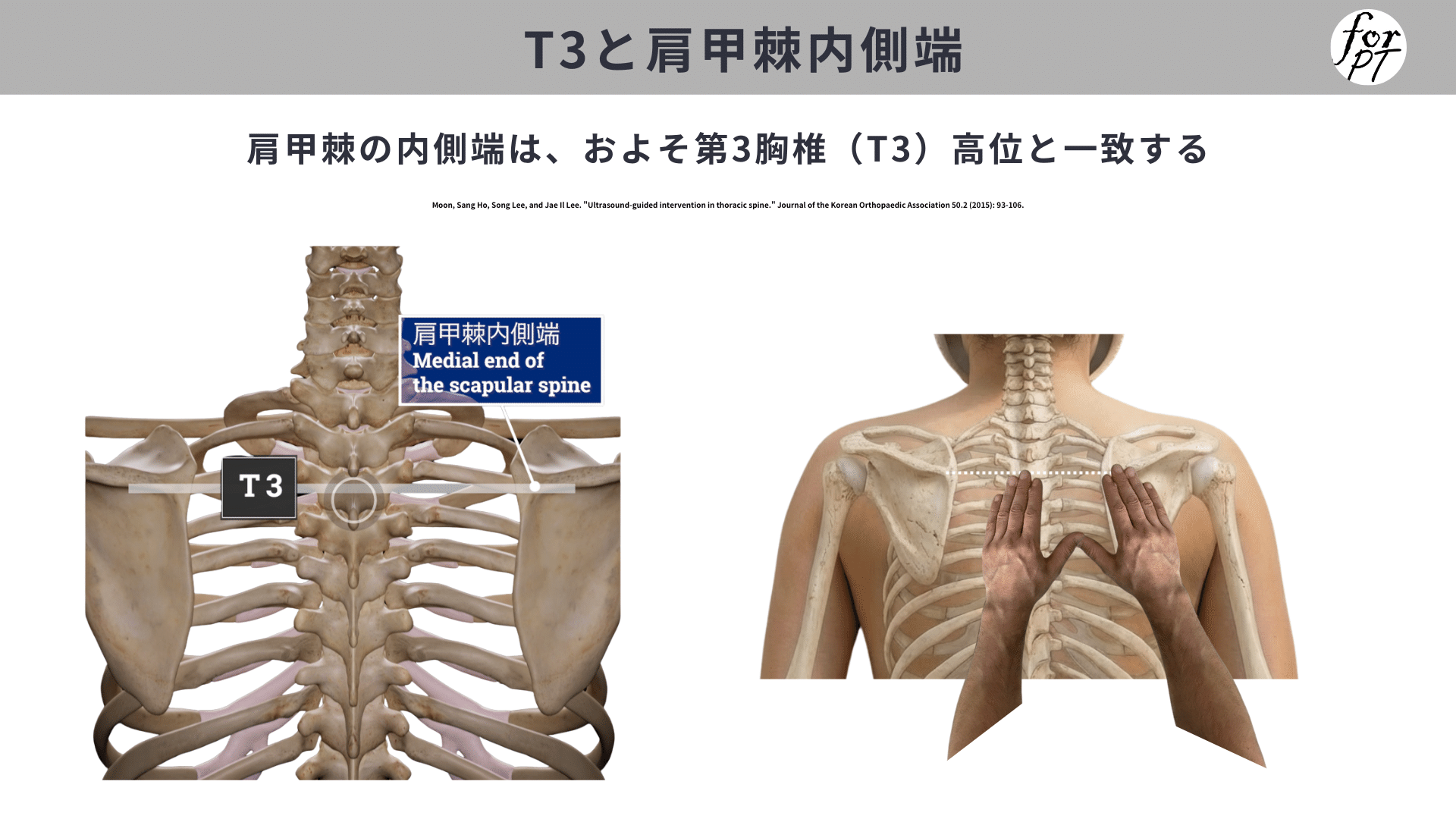
図5 肩甲棘内側端とT3
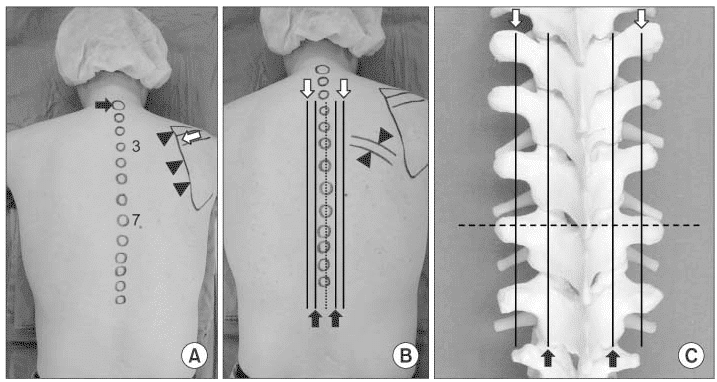
図6 体表からみる肩甲棘内側端とT3の位置(A参照)
3)より画像引用
肩甲骨下角
肩甲骨の下角は、およそ第7胸椎(T7)または第8胸椎(T8)高位と一致する⁴⁾⁵⁾とされます(図7)。
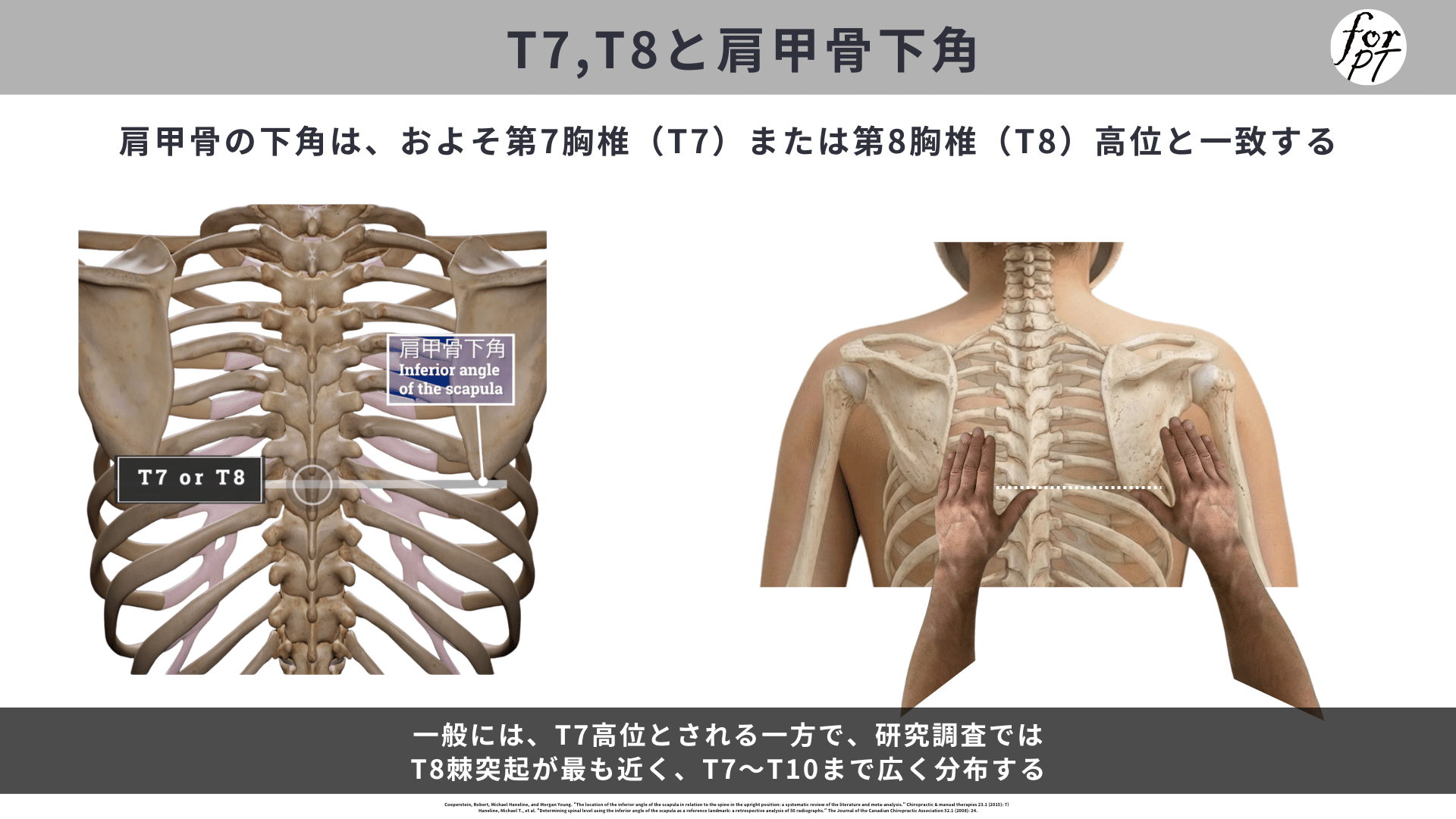
図7 肩甲骨下角とT7・T8
一般には、T7高位とされる一方で、研究調査ではT8棘突起が最も近く、T7〜T10まで広く分布する⁴⁾⁵⁾と報告されています。
肩甲骨内側縁幅
肩甲骨内側縁幅は、第2胸椎から第7胸椎(T2-T7)の高位と一致する³⁾とされています。
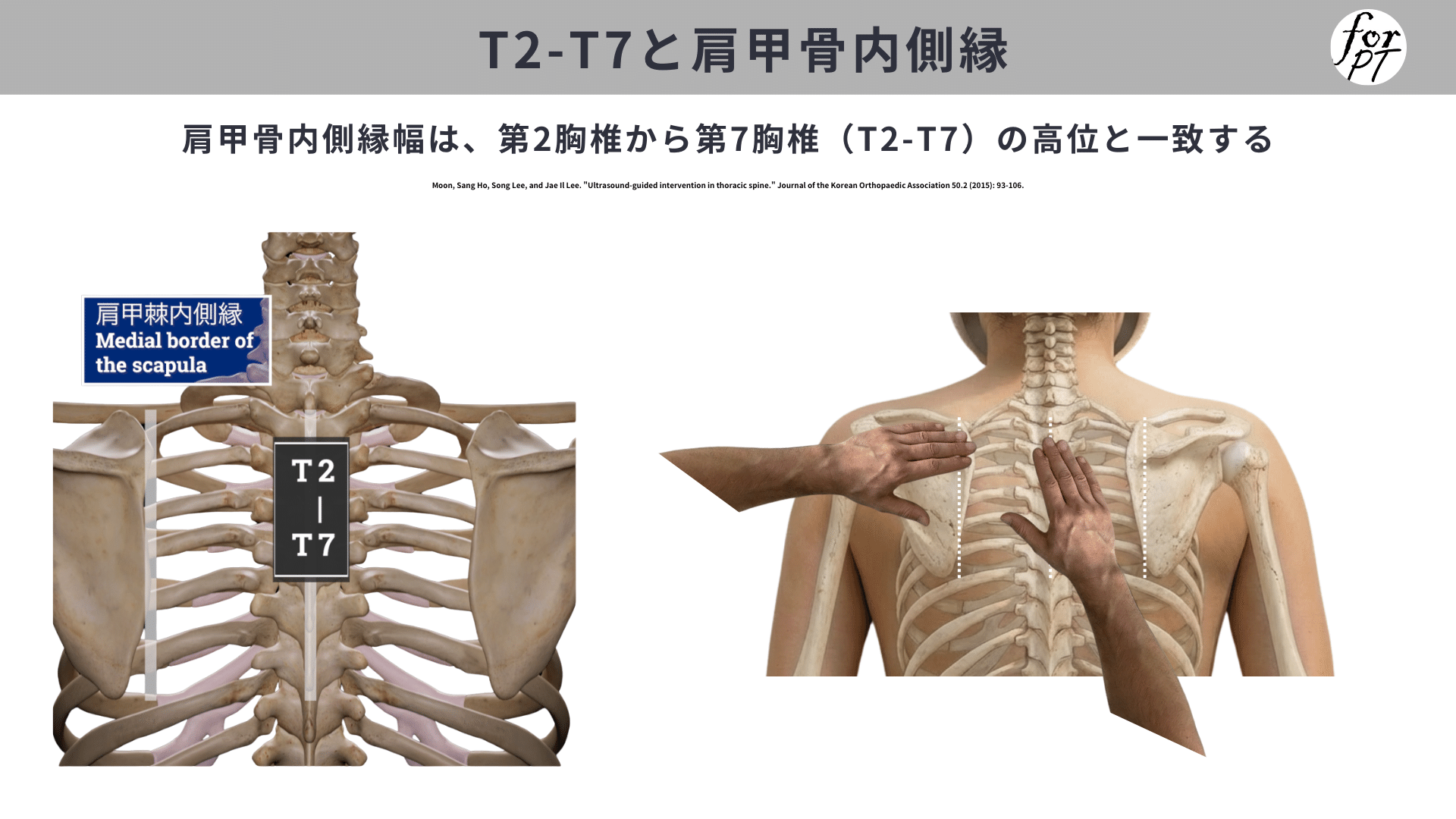
図8 肩甲骨内側縁幅とT2-T7